|
Q.1: “At my site, potential
participants initially show interest in the trial, however, when they
or their family read about the potential bleeding risks, they decline
participation. How can we address these bleeding risks concerns with
participants?”
A: When talking with
potential participants and their families, I emphasise a few points to
ensure that they have a proportionate understanding of the real risk
involved. Firstly – and most importantly – I make it clear that
although rivaroxaban is an anticoagulant, we are using a very low dose
of this medication. It helps to be clear that this is not like
going on warfarin or clopidogrel (which they may have heard of). I
follow this up by reporting that the latest blinded Data and Safety
Monitoring Board report has showed that the observed bleeding rate till
date is actually lower than expected for
patients with advanced CKD and kidney failure. Secondly, I find it
useful to explain that clotting is part of the problem when people have
heart attacks or strokes – and so, like with aspirin, we believe that a
low dose of a blood thinner may shift the balance in the body enough to
reduce the chance of a cardiovascular event, without much increased
risk of bleeding – this is, after all, why we’re doing the study.
Finally, we’re clear that the trial has been designed very carefully to
ensure that patients who are at high risk for major bleeding are
specifically excluded – so if the participant has any particular concern then I want to hear it – I don’t want to
enrol them if they are going to be at higher than expected bleeding
risk.
Q.2: “When discussing the trial,
some participants do not perceive benefits in trial participation. In
their understanding, this is a preventive treatment that will not cure
their diseases. How to clearly explain the potential benefits for the
participants?”
A: I find two approaches
here:
1) Appeal to self-interest – I explain that it is a well-known fact
that the survival rates for patients with advanced CKD and kidney
failure are substantially lower than many commonly diagnosed cancers
such as breast and colorectal cancers. Nearly 50 to 60% of these deaths
are due to cardiovascular disease. Unfortunately, life-saving
medications, including rivaroxaban, that improve cardiovascular
survival are not approved for patients with advanced CKD and
kidney failure as their safety-benefit profile has not been tested
in trials in these patients. Being in the TRACK trial gives the patient
direct access to a treatment that is shown to be beneficial in people
without advanced CKD. Sure, they might get placebo – but why wouldn’t
they want to have a 50% chance of access to a potentially useful
treatment?
2) Appeal to altruism – the data that they provide will help us
determine if this treatment is indeed beneficial. If it is, we will
then be able to use it in many more people and make a real difference
to others who are in the same position that them. Since the burden of
cardiovascular disease is very high among patients with advanced
CKD and kidney failure, 'prevention' of cardiovascular events should be
the top priority.
Q.3: “Some participants have
expressed concern that it is a placebo-controlled trial and if they
receive the placebo that they will be at a disadvantage and therefore
chose not to participate” How can we address participants concern
regarding receiving placebo?”
A: It is important to
tell potential participants that even if they receive a placebo, they
will receive the standard treatment as well. Therefore, the placebo
treatment is not inferior to the standard treatment, and they
are not disadvantaged even if they receive a placebo. In fact, studies
show that trial participants do better than non-trial participants – in
part because they are being watched over by the trial team as well as
their usual doctors. From a purely self-interested point of view,
since placebo is not harmful and the study is pragmatically designed so as to be low burden to them, they may as well
choose to gain a 50% chance of receiving a potentially useful treatment
as the downside of ‘placebo’ is small.
Q.4: “When discussing
the study with my colleagues some have decline to refer any eligible
participants because of concerns around increased bleeding risk. Is
there any data available around perceived increased bleeding risk for
participants in the study”
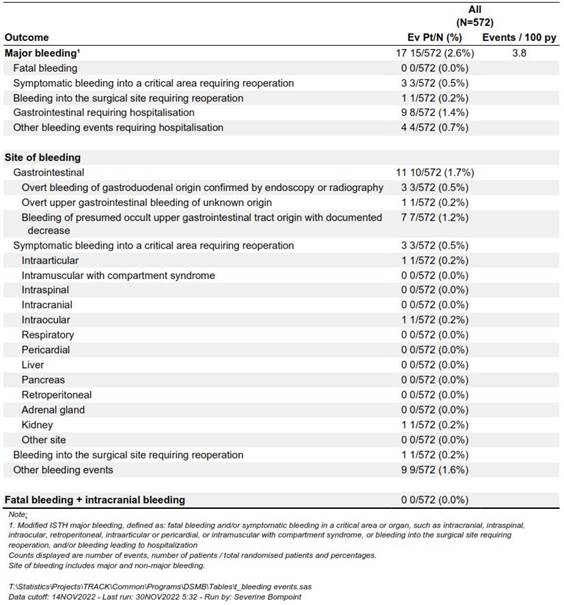
A: There is a wealth of
data to support the low risks associated with low dose rivaroxaban.
According to the latest DSMB (December 2022), the blinded major
bleeding rate in the TRACK trial was 3.8 per 100 person-years. This is
lower than that described in cohort studies (haemodialysis on
antithrombotic treatment 6.7 per 100 person-years and peritoneal dialysis on
antithrombotic treatment 5.7 per 100 person-years: Nephrol Dial
Transplant 2021, 36:170-175), and trials involving therapeutic
anticoagulation (RENAL-AF trial: apixaban 31.5 per 100 person-years and
warfarin 25.5 per 100 person-years; Valkyrie trial: rivaroxaban
9 per 100 person-years and 22.7 warfarin per 100
person-years).
Q.5: “The TRACK trial does not
pay as much per participant as some of our commercial trials so
sometimes there is a reluctance to enrol participants into the study”
Why should we enrol into this trial over other trials?”
A: Although commercial
trials pay a lot more than the TRACK trial, commercial trials are also
labour-intensive with extensive data collection, extensive
trial-specific investigations, and strict timelines for SAE reporting.
In comparison, the TRACK trial is designed as a large simple trial
(LST) with minimal data collection; full integration of study visits in
routine clinic practice; no extra burden on patients, care-givers and investigators; no requirement for
reporting SAEs within 24 hours (except SUSARs); and no designated
trial-specific laboratory, radiological or cardiac investigations. The
per-participant payment in TRACK is actually
equivalent to commercial trials when adjusted for workload.
|